
In my years as a sex therapist, one belief walked into my office more often than almost any other — usually carried by a woman who’d half-decided something was wrong with her. The belief was this: everyone else orgasms from penetration, and I can’t, so I must be broken.
I want to start by dismantling that, because it’s both extremely common and almost entirely backwards. The inability to reliably orgasm from penetration alone isn’t a malfunction. It’s the statistical norm. And once you understand the anatomy and the research behind it, the whole framing of “something’s wrong with me” tends to dissolve — which is usually the moment things actually start to improve.
So let’s go through what the science actually says. Not the mythology we all absorbed, the science. It’s more reassuring, and frankly more useful, than the stories most of us were handed.
The pleasure gap, in plain numbers
Let’s name the pattern first. When researchers study how reliably people orgasm during partnered heterosexual sex, they find a large, consistent gap: men orgasm in the vast majority of encounters, women in considerably fewer. Large-scale studies on the orgasm gap have documented this repeatedly.
Here’s the part that matters: the same research shows the gap shrinks dramatically in two situations — when sex reliably includes clitoral stimulation, and when women feel able to communicate about what they want. And women report no such “difficulty” when they masturbate. The broader data on this is worth seeing.
Sit with that for a second, because it rearranges everything. If the gap vanishes during masturbation and narrows sharply with clitoral stimulation, then the issue was never female anatomy being mysterious or difficult. The issue is a script — a cultural model of sex that centers penetration and treats everything else as optional warm-up. Scripts can be rewritten. Anatomy can’t, which is why this is good news.
Female anatomy 101: what the science revised
A lot of what many of us learned about female anatomy was incomplete, and some of it was simply wrong. Three corrections matter most here.
The “G-spot” is part of the clitoris. The clitoris is not the small external button most diagrams reduce it to — it’s a much larger internal structure extending several centimeters inside, surrounding the vaginal canal. What people call the “G-spot” is best understood as internal clitoral tissue being stimulated through the vaginal wall. It was never a separate organ.
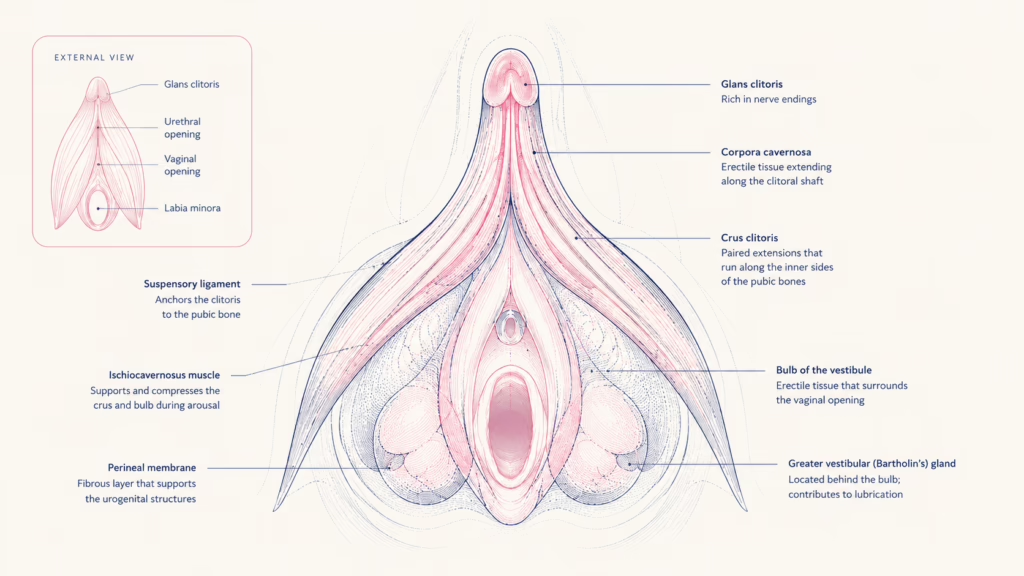
There’s no meaningful “vaginal vs. clitoral orgasm” distinction. This division has caused decades of unnecessary anxiety. Physiologically, the clitoris is involved either way. The idea that a “mature” orgasm should come from penetration alone is a cultural inheritance — traceable in part to outdated psychoanalytic theory — not a finding from modern sexual science.
Direct external clitoral stimulation is reliable for most women. Because the most densely nerve-rich part of the clitoris is external, direct stimulation there is, for most women, the most dependable route to orgasm. This isn’t a workaround. It’s the main road.
The neuroscience of orgasm
Briefly, because it’s genuinely fascinating and it reframes “desire” as something physiological rather than a matter of willpower.
Dopamine drives anticipation and wanting — the build-up, the pursuit. Oxytocin surges around orgasm and is tied to bonding and connection. Endorphins produce the warm, relieved afterglow. And brain-imaging research has found something striking: at the point of orgasm, regions associated with anxiety, judgment, and self-monitoring quiet down.
That last finding is, I think, the most clinically useful thing in this entire article. It means a brain preoccupied with stress, self-consciousness, or “am I doing this right” is working directly against arousal. Which is exactly why mental state turns out to matter as much as technique.
Why penetration alone isn’t enough for most women
Putting the anatomy and the data together, the conclusion is simple and not at all a criticism of anyone: penetration alone stimulates the external clitoris only indirectly and inconsistently. For most women, most of the time, that’s not enough to reliably reach orgasm. This is normal. It is not a flaw in you or your partner. It’s how the bodies are built.
The practical implication is liberating rather than limiting: sex designed around clitoral stimulation — by hand, by mouth, with a toy, in whatever combination works — isn’t “settling” for an alternative. It’s working with the anatomy instead of against it.
The role of mental state
Desire isn’t purely mechanical, and the dual control model in sex research captures this well: arousal is a balance between an accelerator (things that turn you on) and a brake (things that shut desire down — stress, anxiety, distraction, feeling judged). For many women, the brake is the bigger factor. You can do everything “technically right” and get nowhere if the brake is fully engaged.
This is why stress has such a direct effect on libido — it’s not in your head in the dismissive sense; it’s in your head in the literal, physiological sense. Research on mindfulness and sexual function bears this out: women who practice being present during sex report measurable improvements in arousal and satisfaction.

In practice, this means a good intimate life is built as much on safety, presence, and low-stress conditions as on any particular technique. The brake matters more than the accelerator.
How research is reshaping toy design
One reason all of this has reached the mainstream is that product design finally caught up with the anatomy. Air-pulse / clitoral suction technology was developed specifically around how the external clitoris responds. Pressure-wave and dual-stimulation designs reflect the understanding that combined stimulation often works best. And there’s been a deliberate shift toward smaller, gentler “first” toys for people new to all of this.
If you’re curious about putting any of this into practice, our complete beginner’s guide to using a vibrator is the place to start, and these are the science-informed picks our editors actually recommend.

Air-Pulse Suction Vibrator
Why it fits the science: Built around the external clitoris — exactly
where the research points. Uses air pulses rather than vibration,
designed for the most nerve-rich area we covered above.

Mini Bullet Vibrator
Why it fits the science: Simple, precise external stimulation —
the most dependable route for most women, as the anatomy explains.
A low-pressure place to start.
A final note
If you’ve spent years quietly believing your body doesn’t work the way it’s “supposed to,” I hope this is the article that retires that belief for good. The research is unusually clear and unusually kind here: the most common pattern is not a problem, the anatomy is not mysterious, and the thing most likely to be getting in the way isn’t your body — it’s a script nobody chose and the stress nobody needs.
Understanding how it actually works is, more often than not, the beginning of it working better.
Q: Why can’t most women orgasm from penetration alone?
A: Most women need direct clitoral stimulation; penetration reaches the clitoris only indirectly, so it’s the statistical norm not to orgasm from intercourse alone.
Q: Is there a difference between a vaginal and clitoral orgasm?
A: Modern research finds no meaningful physiological distinction — the clitoris is involved either way, since its internal structure surrounds the vaginal canal.
Q: What is the orgasm gap?
A: The documented gap between how often men and women orgasm in partnered heterosexual sex, driven mainly by sexual scripts rather than anatomy.
Q: Is it normal to need clitoral stimulation to orgasm?
A: Yes — it’s the norm, not a problem. The clitoris’s most nerve-rich area is external, making direct stimulation the most reliable route for most women.


